

Abstract
Background: Hepatocytes produce a variety of clotting and fibrinolytic factors. In chronic liver disease (CLD), biosynthesis of these factors is often altered leading to hemostatic aberrations. Recently, the usefulness of PT/INR - one of the five parameters used in the Child-Pugh (CP) scoring system - has been questioned. In this retrospective study, we explored the patterns of plasma alterations relative to CP scores to establish a plasma-based panel that can help evaluate the extent of CLD severity without the use of PT/INR and/or such parameters as the extent of ascites and hepatic encephalopathy.
Methods: Blood was collected via venipuncture (0.129 mol/l sodium citrate) from CLD patients suffering from cirrhosis due to untreated HCV and/or excessive alcohol consumption, that were previously assigned a CP score: CP-A, n=12; CP-B, n=19; CP-C, n=11. Healthy control subjects (n=30) were age and sex matched; all subjects gave informed consent. Within 2 h post-collection, specimens were centrifuged for 15 min at 1500 x g, and then 13000 x g for 2 min to obtain plasma that was immediately frozen at -80°C until used. The following was measured: pro-coagulant phospholipid, fXa, D-dimer, fVIII, sP-selectin, thrombomodulin, protein C, protein S, alternatively spliced Tissue Factor (asTF), free TFPI, TF/TFPI ratio, and TFPI/protein S ratio. Thrombin generation tests (TGT) with and without thrombomodulin were performed. To interrogate the biology of CLD, patient plasma was also analyzed for the levels of microvesicles (MVs) of various origin: endothelium (CD31+/CD41-), monocytes (CD14+), leukocytes (CD11b+), neutrophils (CD16+), platelets (CD41a+, CD41a+/CD62P+, CD62P+), and exosomes (CD63+). Platelet counts and the levels of Annexin V+ MVs were also evaluated. Results were analyzed using GraphPad Prism v.6.03, and the parameters that were significantly different between control and CLD plasma were further evaluated. A system was developed with specified cutoffs for each parameter, derived using clinically normal ranges as well as the data generated in this study, to compile a composite score for CLD severity.
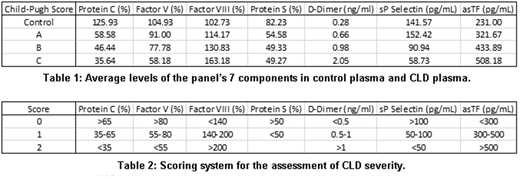
Results: CLD plasma had endogenous thrombin potential comparable to that of control plasma; however, the rate of thrombin generation and peak thrombin generation diminished with increased CLD severity (both p < 0.0001), prolonging the time until peak (p < 0.01) as assessed by TGT. Of the 14 remaining parameters investigated in CLD and control plasma, the levels of fVIII, D-dimer, and asTF increased with CLD severity while protein C, fV, protein S, and sP-selectin levels decreased (Table 1) and in combination, these 7 parameters were able to predict the previously assigned CP scores with high accuracy. Our scoring system assigns a numeric value (0, 1, or 2) for each parameter; a cumulative score of <2 is normal, 2-3 CP-A, 4-7 CP-B, and ≥8 CP-C (Table 2). The system was 97.2% accurate at predicting the CP score: of the 72 plasma samples analyzed, there was only one false positive (a control scored as a CP-A), and one CP-C sample scored as CP-B. Omission of any of the 7 components markedly lowered the system's accuracy. Levels of CD31+/CD41-, CD62+, CD63+, and CD16+ MVs rose with disease severity (p < 0.0001 for all) while CD41a+ MVs decreased (p < 0.0001). Of the panel's 7 components, asTF is relatively novel and so asTF's association with various markers was further examined. There was a positive correlation between asTF and D-dimer (r = 0.305, p = 0.05) and asTF and CD63 (r = 0.346, p = 0.025); asTF negatively correlated with CD14+ MVs (r = -0.348, p = 0.024). There was a strong and highly significant positive correlation between asTF and CD31+/CD41- MVs (r = 0.630, p = 7.81x10-6).
Conclusions: Here we report a novel plasma panel with potential utility in assessing CLD severity in a point-of-care setting. Our scoring system exhibits 97.2% accuracy and does not require clinical assessment beyond plasma analysis. asTF levels positively correlate with those of CD31+/CD41- MVs and both increase with CLD severity; this is in agreement with earlier reports of inflammatory cytokines eliciting asTF secretion from endothelial cells. Larger-scale prospective studies are warranted to validate our findings.
No relevant conflicts of interest to declare.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal